How Long to Retain HIPAA Records: A Clear Guide
Join thousands of professionals and get the latest insight on Compliance & Cybersecurity.
You've set up your healthcare practice with all the right HIPAA safeguards in place. Your team is trained, your systems are secure, and your privacy notices are displayed. But when it comes to how long you need to keep all these records, confusion sets in. You might have heard that "HIPAA requires a six-year retention period," but also that "there are no HIPAA retention requirements for medical records." Surprisingly, both statements are correct.
This contradiction leaves many healthcare professionals scratching their heads, wondering which rules apply to which documents, and how to avoid costly violations that can range from $137 to $68,928 per incident.
The key to compliance lies in understanding a critical distinction that isn't always clearly communicated: the difference between HIPAA compliance documentation and actual patient medical records.
The Critical Distinction: HIPAA Documentation vs. Medical Records
The most common misconception about HIPAA is that it establishes a universal retention period for all health-related documents. This is incorrect. The rules differentiate between documentation related to HIPAA compliance and the patients' medical records themselves.

The HIPAA Six-Year Rule Explained
The Health Insurance Portability and Accountability Act (HIPAA) mandates that specific administrative, technical, and physical safeguard documentation must be retained for a minimum of six years.
As stated in the HIPAA Administrative Simplification regulations, this retention period starts from the date of the document's creation or the date when it was last in effect, whichever is later. This "last in effect" clause is crucial; if a policy is updated, the old version must still be kept for six years from its retirement date. The legal basis for this requirement is found in the Code of Federal Regulations, specifically 45 CFR §164.316(b)(1).
What Documents Fall Under the Six-Year Rule?
Covered Entities and their Business Associates must retain the following types of documents for six years:
- Policies and Procedures: All versions of your organization's privacy and security policies.
- Notices of Privacy Practices (NPPs): Both current and past versions provided to patients.
- Risk Assessments and Risk Analyses: Documentation of your periodic security risk evaluations.
- Authorizations for PHI Disclosure: Signed patient consents for disclosing their Protected Health Information.
- Business Associate Agreements (BAAs): Contracts with vendors must be retained for six years after the termination of the agreement.
- Workforce Training Documentation: Records proving that staff have received HIPAA training.
- Incident and Breach Notification Documentation: All records related to security incidents and any subsequent breach notifications.
- Complaint and Resolution Documentation: Records of any PHI-related complaints and how they were resolved.
- IT Security and Access Logs: System audit logs and access reports.
This list is not exhaustive, but it covers the primary categories of compliance documentation that must be retained under HIPAA regulations.
Medical Record Retention: A Matter of State Law
Here's where the confusion often arises: HIPAA itself does not define how long a provider must keep a patient's medical records. This responsibility is deferred to individual state laws, which leads to significant variation across the country.
Examples of State-Level Medical Record Retention Requirements
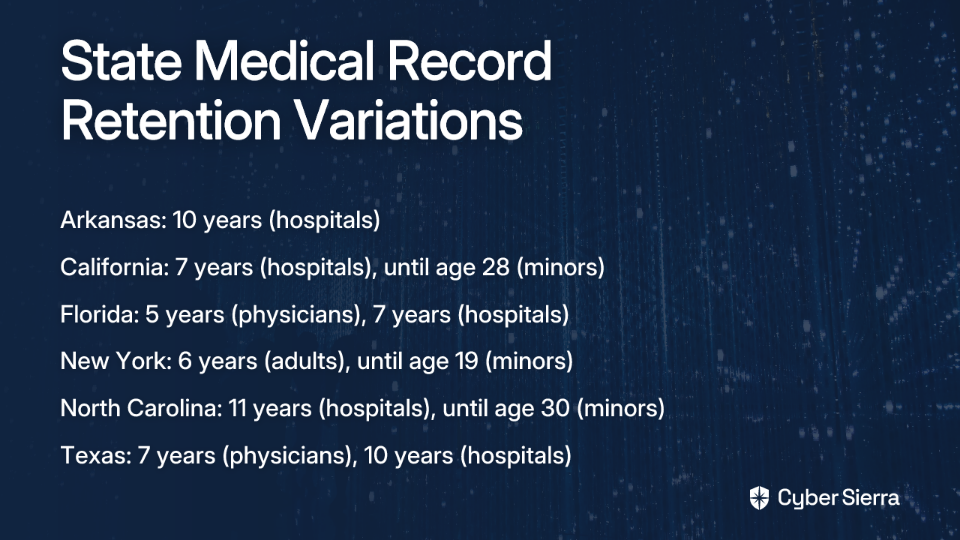
The retention periods can vary significantly, not just by state but also by the type of facility (hospital vs. physician's office) and patient age (adult vs. minor).
- Arkansas: Hospitals must retain records for 10 years; the master patient index must be kept permanently.
- California: Physicians must retain records for 6 years; hospitals for 7 years post-discharge. For minors, records must be kept until they turn 28.
- Florida: Physicians retain records for 5 years from the last patient contact; hospitals for 7 years.
- New York: Adult records are kept for 6 years; minors' records are kept until one year after they reach the age of 18 (i.e., age 19), or 6 years, whichever is longer.
- North Carolina: Hospitals must keep records for 11 years. For minors, records must be retained until the patient reaches age 30.
- Texas: Physicians retain records for 7 years; hospitals for 10 years post-discharge. For minors, records are kept until the patient turns 20.
It is crucial for every Covered Entity and Business Associate to research and document the specific laws for the state(s) in which they operate. The Office of the National Coordinator for Health Information Technology (ONC) provides guidance and resources to help navigate these state-specific requirements.
Juggling Regulations: When HIPAA, State, and Federal Laws Overlap
A common point of confusion is what to do when different laws prescribe different retention periods. HIPAA's regulations include a "preemption" clause. In practice, this means you must follow the stricter law that provides greater privacy protection or longer retention. If your state requires medical records to be kept for 10 years, you must follow that 10-year rule, as it is more stringent than HIPAA's 6-year rule for compliance documents.
Other Overlapping Regulations
Compliance doesn't stop with HIPAA and state laws.
- Centers for Medicare & Medicaid Services (CMS): Healthcare providers who treat Medicare patients have additional obligations. CMS requires that providers retain patient medical records for a period of 5 years, and financial records, such as cost reports, for at least 10 years after the cost report is filed.
- Financial Industry Regulatory Authority (FINRA): Health insurance companies may be subject to FINRA rules which could require indefinite retention of certain records.
How long must HIPAA compliance records be retained? The answer depends on multiple layers of regulations, with the six-year HIPAA requirement serving as just the federal baseline for compliance documentation. For actual medical records, you must refer to your state's laws, which typically range from 5-10 years for adults and often longer for minors.

The Final Step: Secure Disposal of Records
Once a retention period has expired, you cannot simply throw records away. HIPAA requires that PHI be rendered unreadable, indecipherable, and otherwise unable to be reconstructed. Improper disposal is a HIPAA violation that can result in significant penalties.
Acceptable Disposal Methods
For Paper Records, acceptable methods include:
- Shredding (preferably cross-cut)
- Burning
- Pulping
- Pulverizing
For Electronic Protected Health Information (ePHI), methods must ensure data is permanently destroyed:
- Clearing: Using software to overwrite data with non-sensitive data.
- Purging: Degaussing or exposing the media to a strong magnetic field to disrupt the recorded magnetic domains.
- Physical Destruction: Incinerating, melting, pulverizing, or shredding electronic media like hard drives, SSDs, backup tapes, and CDs.
Using a Third-Party Disposal Vendor
It is permissible to hire a third-party service for record destruction. However, this vendor is considered a Business Associate, and you must have a signed Business Associate Agreement (BAA) in place that outlines their responsibilities for protecting PHI during the disposal process.
Best Practices for a Compliant Data Retention Program
To effectively manage these complex requirements, organizations should implement a formal data retention program with the following components:

- Develop a Formal Retention Policy: Document the specific retention periods for all types of data you handle, including HIPAA compliance documents, medical records (per state law), and financial records (per CMS).
- Appoint a Privacy and/or Security Officer: Designate a specific individual or team responsible for overseeing, implementing, and updating the retention policy.
- Conduct Regular Audits: Routinely audit your systems and processes to ensure policies are being followed correctly for both record storage and disposal.
- Provide Ongoing Staff Training: Ensure all employees understand their roles and responsibilities regarding data retention and disposal.
- Vet Your Software and Vendors: Ensure any software used for Electronic Health Records (EHR) or document management is HIPAA compliant. Have BAAs in place with all relevant vendors.
- Maintain Meticulous Documentation: Keep a log of when records are destroyed, including the date, method of destruction, and a description of the records. This documentation is your proof of compliance.
Conclusion
Navigating data retention requires a clear understanding of the rules. Remember the core principles:
- How long must HIPAA compliance records be retained? The answer is six years for documentation related to HIPAA compliance, not for medical records themselves.
- State laws dictate the retention period for patient medical records, and these vary widely, often between 5-10 years for adults and longer for minors.
- Always adhere to the most stringent applicable law (State, HIPAA, CMS, etc.).
- Secure, documented disposal is just as important as retention.
A proactive, well-documented data retention policy is not just a compliance checkbox; it is a fundamental component of protecting patient information and safeguarding your organization from significant legal and financial risk. By understanding the distinction between HIPAA compliance documentation and medical records, and by researching your state's specific requirements, you can develop a retention strategy that meets all applicable regulations while protecting both your patients and your practice.

Frequently Asked Questions (FAQ)
What is the HIPAA six-year retention rule for?
The HIPAA six-year retention rule applies specifically to documentation related to your HIPAA compliance efforts, not to patient medical records. This includes items like your policies and procedures, risk assessments, staff training records, Notices of Privacy Practices, and Business Associate Agreements. These documents must be kept for a minimum of six years from their creation date or the date they were last in effect, whichever is later.
How long do you have to keep patient medical records?
The retention period for patient medical records is determined by individual state laws, not by HIPAA. These state-level requirements vary significantly, typically ranging from 5 to 10 years for adults. For minors, the retention period is often much longer, sometimes until they reach a specific age like 28 or 30. You must research and follow the specific laws for the state in which you operate.
What should you do if state and HIPAA retention laws conflict?
When different regulations have conflicting requirements, you must always follow the stricter law that offers greater patient privacy or mandates a longer retention period. For example, HIPAA's six-year rule for compliance documents is a federal minimum. If your state requires you to keep certain patient authorizations (a type of compliance document) for seven years, you must adhere to the seven-year state requirement because it is more stringent.
How must you dispose of medical records once the retention period ends?
HIPAA requires that all Protected Health Information (PHI), whether on paper or electronic, must be destroyed in a way that it becomes unreadable, indecipherable, and cannot be reconstructed. For paper records, this means shredding, burning, or pulping. For electronic records (ePHI), secure methods include clearing (overwriting), purging (degaussing), or physical destruction (shredding, incinerating) of the storage media. Simply deleting files or throwing records in the trash is a violation.
Why is a Business Associate Agreement (BAA) necessary for record disposal?
A Business Associate Agreement (BAA) is required because any third-party vendor you hire to destroy records is considered a Business Associate under HIPAA. The BAA is a legally binding contract that ensures the vendor will handle and dispose of the Protected Health Information (PHI) with the same level of security and privacy that your organization is required to. This protects your practice by formally outlining the vendor's responsibilities for safeguarding patient data during the destruction process.